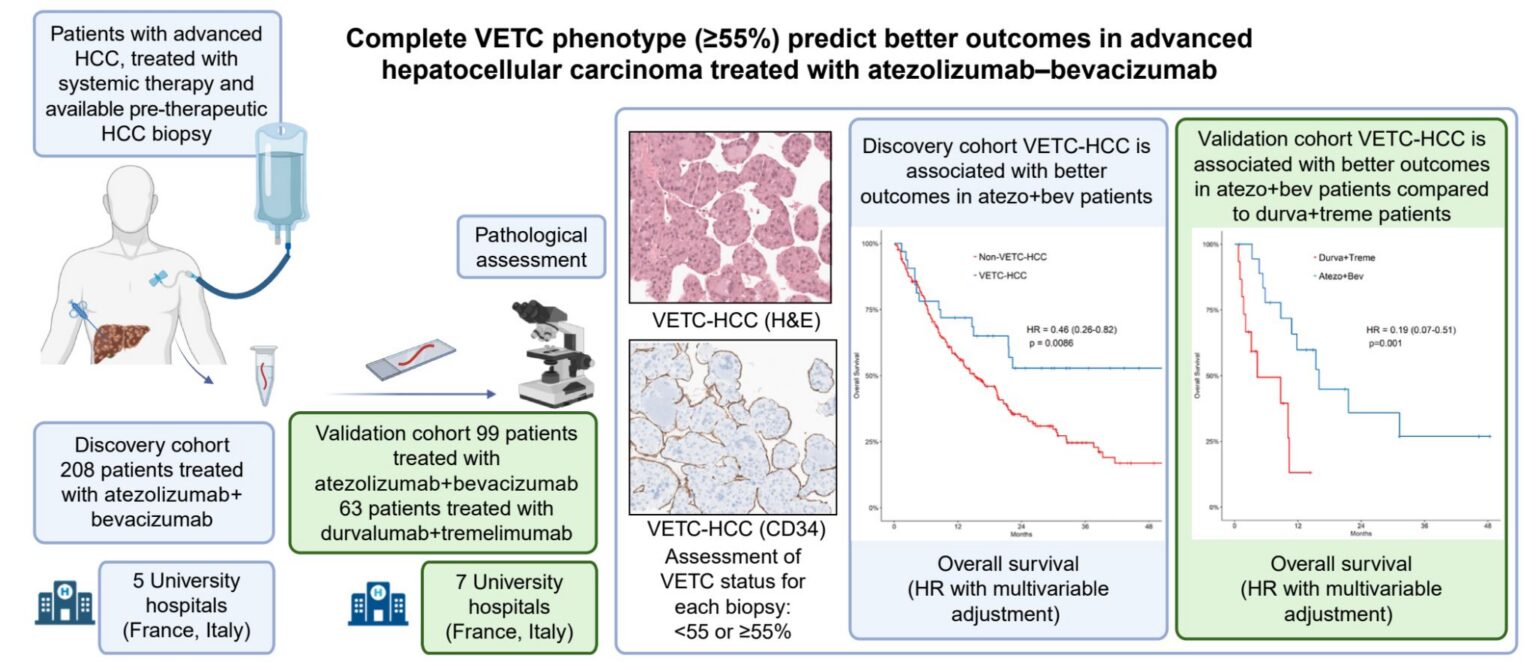

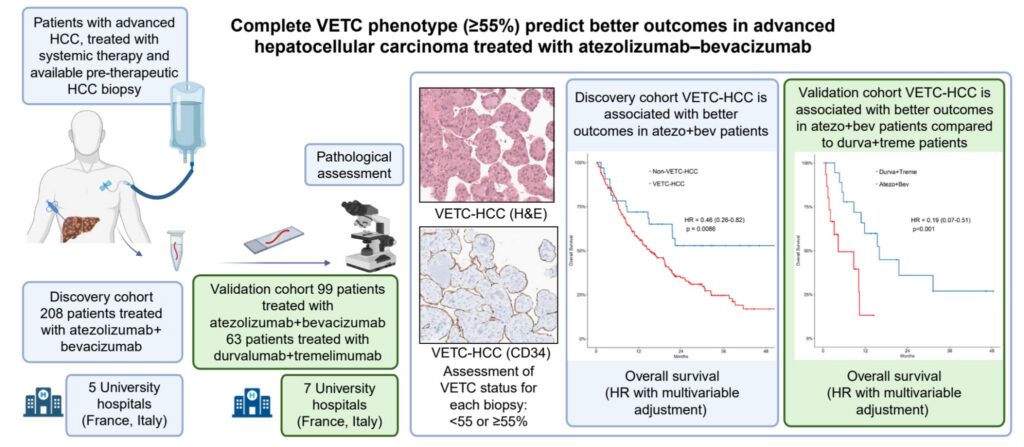
In this French–Italian cohort, the VETC phenotype was predictive of improved outcomes in patients treated with atezolizumab–bevacizumab, with longer survival than patients treated with durvalumab-tremelimumab.
Our findings suggest that VETC represent a promising biomarker for treatment stratification in advanced HCC. Prospective validation studies are now needed to determine whether VETC status could help guide the choice between systemic therapies in routine clinical practice.
Background & Aims
Atezolizumab + bevacizumab and durvalumab + tremelimumab are the standard first-line therapies for advanced hepatocellular carcinoma (HCC). Histological variables routinely associated with outcomes remain poorly described. We aimed to assess the prognostic and predictive value of the vessels encapsulating tumor clusters (VETC) phenotype in this setting.
Methods
We retrospectively analyzed 208 patients in a discovery cohort with advanced HCC treated with atezolizumab + bevacizumab and available pre-treatment biopsies, and 163 patients in a validation cohort, including 99 treated with atezolizumab + bevacizumab and 64 with durvalumab + tremelimumab. In addition to baseline clinico-biological variables, we assessed histological features, including the VETC phenotype, defined as complete (≥55% of tumor area), or incomplete (1–54% of tumor area). Prognostic impacts were evaluated using multivariable Cox models.
Results
In the discovery cohort, the complete VETC phenotype (n = 32) displayed the highest objective response rate in the cohort (66% vs. 37% in non- or incomplete VETC-HCC, p = 0.002), according to the modified RECIST. The complete VETC phenotype was independently associated with better progression-free survival (PFS) (hazard ratio [HR] 0.42, 95% CI 0.26–0.69, p <0.001) and overall survival (OS) (HR 0.46, 95% CI 0.26–0.82, p = 0.008). In the validation cohort, complete VETC-HCC was associated with worse outcomes in patients treated with durvalumab + tremelimumab (PFS: HR 2.44, 95% CI 1.12–5.29, p = 0.024; OS: HR 3.90, 95% CI 1.66–9.15, p = 0.002). Patients with complete VETC-HCC and treated with atezolizumab + bevacizumab had longer survival than patients with complete VETC-HCC and treated with durvalumab + tremelimumab (PFS: HR 0.43, 95% CI 0.17–1.06, p = 0.07; OS: HR 0.19, 95% CI 0.07–0.51, p = 0.001).
Conclusions
We identified complete VETC as a potential predictive marker of outcomes in patients with advanced HCC and treated with atezolizumab + bevacizumab or durvalumab + tremelimumab. Prospective validation of these findings is warranted.